Int. J.
Life. Sci. Scienti. Res., 4(2): 1703-1706, March 2018
Association
of Serum MMP 9 Level with COPD and Healthy Control in North Indian
Population
Sarika Pandey1*, Priyanka
Gaur2, Rajiv Garg1,, Surya Kant1, Sandeep Bhattacharya2,
Abhishek Dubey1, Zameerul
Hasan1
1Department of Respiratory Medicine, King
George’s Medical University, Lucknow, Uttar Pradesh,
India
2Department of Physiology, King George’s Medical
University, Lucknow, Uttar Pradesh, India
*Address for Correspondence:
Ms. Sarika Pandey, Ph.D. Scholar, Department of
Respiratory Medicine, King George’s Medical University, Lucknow-
226010, Uttar Pradesh, India
ABSTRACT- Background: Chronic Obstructive pulmonary disease (COPD) is
an increasing cause of morbidity and mortality world-wide. MMP 9 is an acute
phase reactant secreted by the liver in response to infection, inflammation or
tissue damage.
Objectives: Aim of the study was to
evaluate the levels of MMP-9 in the serum of COPD patients and healthy controls
and its association with severity.
Methods: This case-control study was conducted on 35
healthy controls and 40 COPD patients at a tertiary care hospital in north
India. MMP 9 levels were measured in serum by ELISA Kit.
Results:
The present study showed that mean MMP 9 levels in serum was significantly
higher in COPD group as compared to control group (p<0.0001) and the levels increased with the increasing
severity of the disease.
Conclusion: Our study confirms that MMP 9 levels were
significantly higher in COPD patients as compared to controls and their levels
increased with the increasing severity of the disease. Measuring MMP 9 levels
in combination with other biochemical markers can be helpful in monitoring
disease outcome and management of the disease.
Keywords:
COPD, MMP 9, Inflammation, Matrix metalloproteinases
(MMPs)
INTRODUCTION- Chronic
obstructive pulmonary disease (COPD) is a leading cause of morbidity and
mortality worldwide. Smoking and biomass exposure, along with genetic
predisposition, are the major risk factors for developing COPD [1]. Persistent systemic
inflammation and oxidative stress are common features of this disease [2].
Progressive destruction of the extracellular matrix of lungs by MMPs is observed
in chronic obstructive pulmonary disease as well as in the
pathogenesis of other diseases [3].
MMP-9 also known as gelatinase B is 85 kD protein secreted by bronchial
epithelial cells, neutrophils, eosinophils,
mast cells and alveolar macrophages. Increased expression of MMP-9 by inflammatory cells
e.g. neutrophils and macrophages are correlated with
a variety of processes that cause lung damage [4] .
It is thought to have an important role in lung remodeling
and has been investigated as a potential biomarker of COPD. Diagnosis of COPD
is confirmed by spirometry but it depends mainly on
the level of effort done by the patient and so this may alter the diagnosis in
many patients. Therefore study on biomarkers that can be easily measured in peripheral
blood and which can correlate with measures of disease progression is very
promising.
Therefore, with this aim the present study was done in
North Indian COPD patients to evaluate the level of MMP-9 in serum and study its
association with severity as well as other parameters so that there may be other
surrogate method along with FEV1 that can help clinicians in better
understanding the stage of disease and its proper management.
MATERIAL AND METHODS
Study population and selection of subjects- The
present case control study was carried out in the department of respiratory
medicine, King George medical university, Lucknow,
India. The
study was approved by the Institutional ethical committee and written
informed consent was obtained from all the subjects.The
study subjects included were diagnosed cases of stable COPD of both genders. Forty COPD patients and 35 healthy controls
were enrolled. The diagnosis of COPD was based on pulmonary
function test which was done in all patients. According to GOLD criteria, COPD
was defined on the basis of the post bronchodilator FEV1/FVC ratio of less than
0.70 and
reversibility to an inhaled bronchodilator in FEV1 <12% or <200ml after
administration of 200 μg Salbutamol
(2 puffs) using a pressurized metered dose inhaler with a spacer. Subjects
reporting with a history of pulmonary tuberculosis, cardiac diseases, ILD,
pregnancy, diabetes, and cancer were excluded from the study.
Patients with any other systemic disease other than COPD were also excluded. A detailed clinical history of respiratory
symptoms was also obtained. Peripheral Blood samples (5ml) were collected from
all patients and healthy controls and centrifuge in order to analyze levels of
MMP-9 in serum. The obtained serum was kept at -80°C until the time of the
analysis. The MMP-9 level was assessed in serum by Elisa method according to
manufacturer protocol.
Statistical analysis- Graph pad PRISM version 6.01 was used for the
analysis of data. All demographic and clinical data were expressed as a mean±standard error of the mean (SEM) and percentage. The
chi-square test was used for categorical data and groups were compared by
unpaired t-test or one-way analysis of variance (ANOVA), p<0.05 were
considered significant.
RESULTS- The
baseline characteristics of the study groups are shown in Table 1. Age of
patients ranged from 35 to 75 years. Mean age of patients was 56.07±8.51 and
that of healthy controls was 54.37±10.66 years respectively. Statistically,
there was no significant difference between groups with respect to age
(P=0.44). In both the groups,
majority of patients were males. Proportions of males were slightly higher in
COPD group (82.5%) as compared to those in controls (74.2%) while females were
17.5 % in COPD group and 25.7% in controls. In COPD group there were 21 smokers
(52.5 %), 6 non-smokers (15%) and 13 ex-smokers (32.5%) in the COPD group while
in control group, there were 16 smokers (45.7%), 9 non-smokers (25.71%), and 6
ex-smokers (17.14%).
Table 1: Demographic profile of COPD patients and
healthy controls
|
PARAMETERS |
COPD (N=40) |
Control (N=35) |
P-value |
|
Age (Yrs) |
56.07 ± 1.8 |
54.37
± 1.37 |
0.44 |
|
Sex Male Female |
33(82.5%) 7(17.5%) |
26(74.2%) 9(25.7%) |
|
|
BMI (kg/m2) |
21.23 ± 0.77 |
24.19
± 0.74 |
0.007 |
|
Gold Stages |
|
||
|
Stage 1 |
0 |
- |
|
|
Stage
2 |
8(20%) |
- |
|
|
Stage 3 |
22(55%) |
- |
|
|
Stage
4 |
10(25%) |
- |
|
|
Smoking history |
|
|
|
|
Smoker |
21 (52.5%) |
16(45.7%) |
|
|
Non smoker |
6 (15 %) |
9(25.71%) |
|
|
Ex-smoker |
13 (32.5) |
6(17.14%) |
|
According to GOLD
criteria, COPD patients were grouped into four stages based on their severity.
There was no patient in stage 1 having mild COPD while there were 8 patients
(20%) in stage 2 (moderate COPD), 22 patients (55%) in stage 3 having severe
COPD and 10 patients (25%) in stage 4 having very severe COPD. Mean value of
serum MMP9 levels were significantly higher in the COPD patients as compared to
healthy controls (P <0.0001) (Fig 1). As the severity of COPD increases the levels of MMP
9 also increases and was highest in very severe COPD patients (Fig. 2).
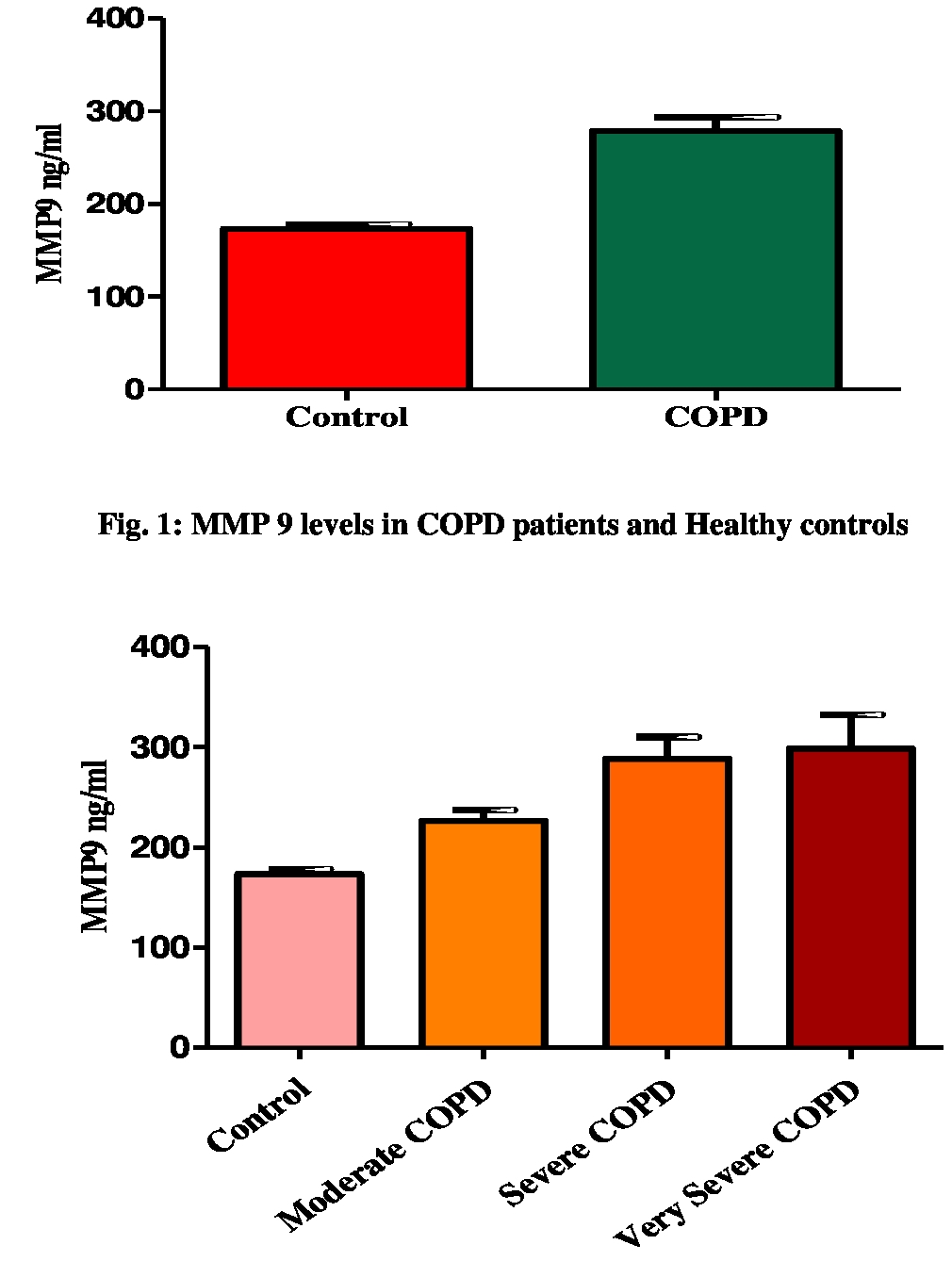
Fig. 2: MMP 9 levels in COPD patients on the
basis of severity according to GOLD
DISCUSSION- Matrix metalloproteinases
(MMPs) are proteolytic enzymes that degrade ECM
components both under physiological conditions and in pathological processes.
(MMP) play a central role in the lung remodeling in
COPD [5-7]. This study, as well as
previous reports, showed that MMP-9 concentrations are associated with airflow
obstruction, suggesting that MMP-9 may play a role in the pathogenesis of COPD.
The present case-control study showed that
serum MMP9 level was significantly higher in the COPD group as compared to
control group (p<0.0001), which was supported by many previous studies [8,9].
the previous study showed that MMP-9 level was
significantly higher in COPD patients when compared to control group and the
levels were higher in severe and very severe stages and this increase could result
in ECM destruction in the airways and contribute in airway remodeling and the decline in lung
function seen in COPD patients [10].
It
has been also found that MMP-9 concentration correlated negatively with the
severity of airway obstruction
(FEV1%, FVC) While Brajer et al. [9] in his study showed that in the COPD group, the MMP-9 levels were
negatively correlated with FEV1 (P=0.01) and FEV1/FVC (P=0.0002) [11].
Study by Linder et al. [12] showed that productive cough and decreasing FEV1
were each associated with MMP-9 in COPD and decreasing FEV1 remained
significantly associated with MMP-9 also after adjustment for common
confounders in this population-based COPD cohort. The increased serum MMP-9
concentrations in COPD indicate an enhanced proteolytic
activity that is related to disease severity. Papakonstantinou
et al. [13] study in BAL
of COPD patients indicate that during AE-COPD increased expression of TIMP-1,
TIMP-2, and MMP-9 and activation of MMP-9 may be persistent aggravating factors
associated with airway remodelling and obstruction, suggesting a pathway
connecting frequent exacerbations to lung function decline. MMP 9 has an
important role in Systemic inflammation in COPD and associated with disease
progression.
CONCLUSIONS- COPD is a multicomponent
disease which affects the physiological conditions and social life of patients.
Our study concluded that MMP 9 level is increased in chronic obstructive
pulmonary disease. Measuring level of MMP 9 in combination with other biochemical
markers will be helpful in monitoring disease outcome in COPD patients and also
in proper assessments, treatment, and management of the disease. The increase
in MMP 9 levels with the progression of the disease as seen reflects the
severity of the disease and so measuring MMP 9 levels at baseline and after
therapy will also prove beneficial for the proper management of the disease.
ACKNOWLEDGEMENTS- We are greatly thankful to Department of Respiratory Medicine and
Department of Physiology for providing necessary facilities for carrying out
the study.We also appreciate the patients and the
healthy volunteers who give their consent for participating in this study.
REFERENCES
1.
Global Initiative for Chronic Obstructive Lung Disease. Global strategy
for the diagnosis, management and prevention of chronic obstructive pulmonary
disease, 2014.
2.
Gopal P,
Reynaert NL, Scheijen JL, Schalkwijk CG, FranssenFM, Wouters EF, Rutten EP.
Association of plasma sRAGE but not esRAGE with lung function impairment in COPD. Respiratory
research, 2014; 15(1):15-24.
3.
Feng L,
Xue D, Chen E, Zhang W, Gao
X, Yu J, Feng Y, PanZ.
HMGB1 promotes the secretion of multiple cytokines and potentiates the
oestrogenic differentiation of mesenchymal stem cells
through the Ras/MAPK signalling pathway. Experimental
and Therapeutic Medicine, 2016; 12(6):3941-7.
4.
Sang QX, Muroski ME, Roycik MD, Newcomer
RG, Van denSteen PE, Opdenakker
G, Monroe HR, Sahab ZJ. Matrixmetalloproteinase-9/gelatinase B is a putative therapeutic target of chronic
obstructive pulmonary disease and multiple sclerosis. Current pharmaceutical
biotechnology, 2008; 9(1):34-46.
5.
Vignola AM, Paganin
F, Capieu L et al. Airway remodeling
assesses by sputum and highresolution computed
tomography in asthma and COPD. Eur Respir J, 2004; 24: 910-917.
6.
Vernooy JHJ, Liendeman
JHN, Jacobs JA, Hanemaaier R, Wouters
EFM. Increased activity of matrix metalloproteinase-8 and matrix
metalloproteinse-9 in induced sputum from patients with COPD. Chest, 2004; 126:1802-1810.
7.
Montano M, Beccerril C, Ruiz V, Ramos C, Sansores RH, Gonzalez-Avilaa G.
Matrix
metalloproteinases activity in COPD associated with wood smoke.
Chest, 2004; 125:
466-472.
8.
Brajer B,
Batura-Gabryel H, Nowicka
A, Kuznar-KaminskaB, Szczepanik
A. Concentration of matrix metalloproteinase-9 in serum of patients with
chronic obstructive pulmonary disease and a degree of airway obstruction and
disease progression. J Physiol Pharmacol,
2008; 59(Suppl 6):145-52.
9.
Xin
XF, Zhao M, Li ZL, Song Y, Shi Y. Metalloproteinase-9/tissue inhibitor of
metalloproteinase-1 in induced sputum in patients with asthma and chronic
obstructive pulmonary disease and their relationship to airway inflammation and
airflow limitation. Chinese journal of tuberculosis and respiratory diseases, 2007;
30(3):192-6.
10. Eman Sobh,
Asmaa Abd AL Salam Almadbouly, Hend Ezzat2, Maha Abd-AllahSerum Levels of
High Mobility Group Box 1 (HMGB1) and Matrix Metalloprotinase
9 (MMP9) are Related to Lung Function Indices in
Chronic Obstructive Pulmonary Disease
Clinical Medicine and Diagnostics, 2017; 7(2):31-39.
11. Beeh
KM, Beier J, Kornmann O,
Buhl R. Sputum matrix metalloproteinase-9, tissue inhibitor of
metalloprotinease-1, and their molar ratio in patients with chronic obstructive
Pulmonary disease, idiopathic pulmonary fibrosis and healthy subjects.
Respiratory medicine, 2003; 97(6):634-9.
12. Linder
R, Rönmark E, Pourazar J, Behndig A, Blomberg A, Lindberg
A. Serum metalloproteinase-9 is related to COPD severity and symptoms -
cross-sectional data from a Population based cohort-study. Respir
Res, 2015; 16(28):1-9.
13. Papakonstantinou et al. Acute exacerbations of COPD are
associated with significant activation of matrix metalloproteinase 9
irrespectively of airway obstruction, emphysema and infection Respiratory
Research, 2015; 16(78):1-12.