Int. J. Life. Sci. Scienti. Res., 4(6):
2080-2087,
November 2018
Knowledge and Practice of Asthmatic’s
Patients Regard using Meter Dose Inhaler
Hassanat
E. Mustafa1*, Mishkat S.A. Rokza2, Badria A. Elfaki3
1Department of
Nursing practices, Umm Al-Qura University, Faculty of Nursing, Makka, Saudi
Arabia, & Al -Neelain University, Khartoum, Sudan
2Department
of Nursing, OmdurmanIslamic University, Khartoum, Sudan
3Department of
Nursing practices, Umm Al-Qura University, Faculty of Nursing, Makka, Saudi
Arabia, & Als-Neelain University, Khartoum, Sudan
*Address for Correspondence: Dr. Hassanat Elbashir Mohammed
Mustafa, Department of Nursing Practices, Umm Al-Qura University, Faculty of
Nursing, P.O.: 715-21955, Makkah AlMakarama, Saudi Arabia
ABSTRACT-
Inadequate management of asthma can lead to physical handicap and death. The
study aimedto assess knowledge and practice of asthmatic participants for use
meter dose inhaler device. A descriptive study involved 105 participants,
conducted at public hospitals in Khartoum state from July to October2014.
Questionnaire and observational check list were used for data collection. The
study enrolled (51%) female and (49%) male. Most of participants their age
group ranged, between 36 to 45 years, (35%) were workers and (31%) received
University education while 44 % had a chronic asthma. Level of participant’s
knowledge was a very good regard care and storage of the device; sequent
(77%-79%). There were(64 %)had moderate level of knowledge for preparation dose
(69%) replacing inhaler device and cleaning mouthpiece (60%), while 56% had
very poor knowledge to rinse mouth after puff. A highly significant difference
between the level of knowledge and education (P value< 0.001) regard
replacing the inhaler device, and cleansing mouthpiece. All participants
demonstrated correct technique of using inhaler device, position, removed,
pressed replacement the cap, shaking inhaler device and took deep breath. While
half of them had moderate skill level for opened mouth technique, continuous
breathing and rinsed mouth after puffuse, and fewer of participants had poor
technique during repeating the puff. Most of participants reflected moderate to
poor level of knowledge and have very good practice for correct used inhaler
meter device; this reveals the discrepancy between knowledge and practice.
Key-words: Asthma,
Knowledge, Meter dose inhaler, Patients, Practice
INTRODUCTION-
Asthma
is a chronic inflammatory disorder of the lung which leads to narrowing of air
passages in response to various triggers, leading to episodes of shortness of
breath and wheezing. The symptoms of asthma can vary greatly in frequency and
severities, ranging from intermittent mild symptoms to an incapacitating and
life-threatening disorder [1]. Worldwide 235-330 million people are
affected by asthma in 2011, and approximately 250,000-345,000 people die per
year from the asthma [2]. The proportion of people with asthma in
United States grew by nearly 15%. In 2009, asthma caused 479,300
hospitalizations, 1.9 million emergency department visits, and 8.9 million
doctor visits [3]. According to the recent report by Global
Initiative for Asthma (GINA); South Africa has the world’s fourth highest
asthma death rate among five to 35 year olds and estimated that 3.9 million in
South Africans with asthma, 1.5% dies of this condition annually [4].
In
Sudan the prevalence of asthma increased from 5% in 2009 and 2010 to 5.6% in 2011
according to the annual reports of the Federal Ministry of Health [5].
Also the prevalence of asthma separately among university students and workers
in Khartoum state was found to be 7.4 % [6]. Inadequate management
of asthma can lead to a significant social and physical handicap and can result
in death due to respiratory failure. Pharmacological therapy is one of the
pillars for proper asthma management [7]. A short burst aerosolized
medicine inhale through Metered Dose Inhalers (MDIs) device that delivers a
specific amount of medication to the lungs; usually self-administered by the
patient [8]. It was first developed in 1950s, and became most widely
used devices for aerosol therapy. Over 70 million patients in the world use a
metered dose inhaler either alone or in association with a spacer [7,8].
Recent study found that more than 60% of
patients were unable to use their MDIs correctly and impact of poor inhaler technique based on the
evidence practice will results in a decreased response to medication and poor
asthma control A large proportion of patients prescribed inhaled medications do
not use their inhalers correctly. Overall, up to 90% of patients show incorrect
technique in clinical studies with standard metered dose inhalers (MDIs) [9].
Incorrect
inhaler practicing technique is common among patients with asthma result in
suboptimal disease control, disability and absences from work in addition to
potential side-effects oral corticosteroid treatment [6] so is
important to know steps and benefits of correct uses of the meter dose inhaler
device [4,10,11]. The purpose of this study to evaluate knowledge
and practice of asthmatic patients regard using of meter dose inhaler to
maximize benefits of oral inhalation medication.
MATERIAL AND METHOD
Descriptive study was conducted at chest
departments of public hospitals at El-Shaab, Omdurman and Abu-Anga in Khartoum
state, Sudan from July to October 2014. Populations of the study were entire
asthmatic patients, who visited or admitted at chest units during the study
period. Non-probability, convenience sampling technique was adopted, sample
size enrolled in this study was 105 subjects which selected based on criteria,
included both genders at age 18 years and above with various qualifications,
occupations and using the meter dose inhaler. While excluded critical asthmatic
cases, children, asthmatic didn't use the meter dose inhaler and patients
disagree to participate. Study variables included background data such as age,
gender, education levels, occupation and duration of the disease, dependent
variables about knowledge about preparation, inhalation steps, storage mouth
rinse, and cleanness and correct practice for uses meter dose inhaler device.
Data was collected using interviewing
and observation techniques. Questionnaire and check list constructed to collect
relevant data for knowledge and practice of participants about meter dose
inhaler device. A structured questionnaire was composed of 13 close-ended
questions, consists of two sections. The first section for the demographic data
and the second section reflect the knowledge of participants regard meter dose
inhaler device. Check list was constructed to identify the practice of
asthmatic patients during uses of meter dose inhaler device in relation to
international guidelines. Pilot study for instruments carried out for sixteen
volunteers prior to commencement of data collection and some correction was
done for questionnaire.
Statistical Analysis-
Data analyzed used statistical program for social sciences (SPSS) version
20after cleaned and coded. Knowledge variables scored according to Liker’s
scale [12] ‘very poor, poor, fair (moderate) good and very good.
Descriptive analysis was made for background variables and results presented
inform of percentage and frequency tables. Chi squire to test differences
between variables such as meter dose inhaler step preparation, storage mouth
rinse, and cleanness in relation to their education level was used and p-value
<0.005 to test significances [13].
The ethical
considerations were granted by ethical clearance from the institutional review
board at Al-Neelain University, officially endorsed by the ethical committee in
El-Shaab, Omdurman and Abu-Anga public hospitals and written consent from
entire participants after explanation and full information.
RESULTS
Table 1 shown characteristics background of 105 participants, (51%)
female and (49%) male. (27%) of participants at age group 36- 45years (35%)
were workers and (31%) with University education, in
addition to (44%) of participants experience asthma for 6 to 15 years.
Table 1: Characteristics back ground of
participants (n = 105)
|
Items |
Frequency |
Percentage |
|
|
Gender |
Male |
51 |
49.0% |
|
Female |
54 |
51.0% |
|
|
Age |
18 – 25 |
13 |
12. 0% |
|
26 – 35 |
24 |
23.0 % |
|
|
36 – 45 |
28 |
27.0% |
|
|
46 – 55 |
26 |
25.0% |
|
|
56 – 65 |
14 |
13.0% |
|
|
Occupation |
Employee |
22 |
21.0% |
|
Student |
14 |
13.0% |
|
|
worker |
37 |
35.0% |
|
|
Other |
32 |
31.0% |
|
|
Level of education |
Illiterate |
15 |
14.0% |
|
Primary |
20 |
19.0% |
|
|
Secondary |
30 |
29.0% |
|
|
Universal |
33 |
31.0% |
|
|
Post universal |
7 |
7.0 % |
|
|
Duration of asthma |
1
– 5 |
27 |
26.0 % |
|
6
– 15 |
46 |
44.0% |
|
|
16
– 30 |
30 |
28.0% |
|
|
Above
30 |
2 |
2.0% |
|
Table
2 reflected knowledge score of
participants who used meter dose
inhaler device; which are very good about steps of inhalation dose, steps of
care post inhalation, storage and clean the device respectively (77%, 44%, 79%,
43%), while participants have moderate level of knowledge about preparation of
the dose, replacement and cleaning mouthpiece with respectively proportions of
63% , 68%, 60% in addition to (52%) of participants have poor knowledge about
benefit of oral rinsing after puff.
Table
2: Level of knowledge among participants regard inhaler medication for
management of Asthma using meter dose inhaler device (n=105)
|
Items |
Very good |
Good |
Fair |
Very poor |
|
Steps of preparation |
34.0% |
0.0% |
64.0% |
2.o% |
|
Steps of dose inhalation |
77.0% |
18 % |
5.0% |
0.0% |
|
Care steps post inhalation |
44.0% |
37.0% |
19.0% |
0.0% |
|
Keeping (Storage) of the device |
79.0% |
7.0% |
14.0% |
0.0% |
|
Benefit of oral rinsing after
puff |
8.0% |
0.0% |
36.0% |
56.0% |
|
Replacement |
30.0% |
0.0% |
68.0% |
2.0% |
|
Mouthpiece cleaning |
18.0% |
0.0% |
60.0% |
22.0% |
|
Device cleaning methods |
43.0% |
21.0% |
14.0% |
22.0% |
Table
3a & b showed a significant differences between levels of knowledge during preparation,
inhalation dose, replacing and cleaning mouthpiece of the meter dose inhaler
device versus level of education; P-values (0.000, 0 .033, 0.001,
0.001sequences), while insignificant differences about steps of inhaler dose,
storage, cleaning of meter inhaler device and rinse of mouth after puff;
P-values (0.203, 0.297, 0.353, 0.242 sequences).
Table
3a: Level of knowledge among participants regard using meter dose inhaler
device versus level of education (n= 105)
|
Items |
Education level |
Level
of knowledge |
Total |
P- value |
|||
|
Steps of preparation |
Very
good |
Good |
Fair |
Very
poor |
|||
|
Illiterate |
7.0% |
0.00% |
93.0% |
0.0% |
100% |
0.000 |
|
|
Primary |
5.0% |
0.00% |
95.0% |
0.0% |
100% |
||
|
Secondary |
44.0% |
0.00% |
50.0% |
7.0% |
100% |
||
|
Universal |
42.0 |
0.00% |
58.0% |
0.0% |
100% |
||
|
Post University |
100.0 |
0.00% |
0.0% |
0.0% |
100% |
||
|
Dose inhalation steps |
Illiterate |
47.0% |
40.0% |
13.0% |
0.00% |
100% |
0.203 |
|
Primary |
75.0% |
20.0% |
5.0% |
0.00% |
100% |
||
|
Secondary |
80.0% |
17.0% |
3.0% |
0.00% |
100% |
||
|
Universal |
88.0% |
9.0% |
3.0% |
0.00% |
100% |
||
|
Post University |
86.0% |
14.0% |
0.0% |
0.00% |
100% |
||
|
Steps follow dose inhalation |
Illiterate |
27.0% |
26.0% |
47.0% |
0.00% |
100% |
0.033 |
|
Primary |
40.0% |
25.0% |
35.0% |
0.00% |
100% |
||
|
Secondary |
50.0% |
43.0% |
7.0% |
0.00% |
100% |
||
|
Universal |
46.0% |
42.0% |
12.0% |
0.00% |
100% |
||
|
Post University |
57.0% |
43.0% |
0.0% |
0.00% |
100% |
||
|
Storage of Meter Dose Inhaler Device |
Illiterate |
80.0% |
7.0% |
13.0% |
0.00% |
100% |
0.297 |
|
Primary |
70.0% |
5.0% |
25.0% |
0.00% |
100% |
||
|
Secondary |
93.0% |
0.0% |
7.0% |
0.00% |
100% |
||
|
Universal |
76.0% |
12.0% |
12.0% |
0.00% |
100% |
||
|
Post University |
57.0% |
14.0% |
29.0% |
0.00% |
100% |
||
Table 3b: Level of Knowledge among
Participants Regard Using Meter Dose Inhaler Device to Control bronchial Asthma
versus Level of Education (n= 105)
|
Items |
Educational
level |
Level of
knowledge |
Total |
P-value |
|||
|
Very good |
Good |
Fair |
Very poor |
||||
|
Cleaning of Meter Inhaler Device |
Illiterate
|
20.0% |
27.0% |
13.0% |
40.0% |
100% |
0.353 |
|
Primary |
25.0% |
35.0% |
15.0% |
25.0% |
100% |
||
|
Secondary |
47.0% |
17.0% |
16.0% |
20.0% |
100% |
||
|
Universal |
55.0% |
15.0% |
12.0% |
18.0% |
100% |
||
|
Post
University |
72.0% |
14.0% |
14.0% |
0.0% |
100% |
||
|
Rinse of mouth after Puff |
Illiterate
|
0.0% |
0.00% |
20.0% |
80.0% |
100% |
0.242 |
|
Primary |
0.0% |
0.00% |
35.0% |
65.0% |
100% |
||
|
Secondary |
13.0% |
0.00% |
34.0% |
53.0% |
100% |
||
|
Universal |
12.0% |
0.00% |
46.0% |
42.0% |
100% |
||
|
Post
University |
0.0% |
0.00% |
43.0% |
57.0% |
100% |
||
|
Replacing the Meter Dose Inhaler
Device |
Illiterate
|
0.0% |
0.00% |
93.0% |
7.0% |
100% |
0.001 |
|
Primary |
10.0% |
0.00% |
90.0% |
0.0% |
100% |
||
|
Secondary |
33.0% |
0.00% |
67.0% |
0.0% |
100% |
||
|
Universal |
39.0% |
0.00% |
58.0% |
3.0% |
100% |
||
|
Post
University |
86.0% |
0.00% |
14.0% |
0.0% |
100% |
||
|
Cleaning Mouthpiece |
Illiterate
|
0.0% |
0.00% |
60.0% |
40.0% |
100% |
0.001 |
|
Primary |
0.0% |
0.00% |
75.0% |
25.0% |
100% |
||
|
Secondary |
17.0% |
0.00% |
63.0% |
20.0% |
100% |
||
|
Universal |
27.0% |
0.00% |
55.0% |
18.0% |
100% |
||
|
Post
University |
71.0% |
0.00% |
29.0% |
0.0% |
100% |
||
Fig.
1 Showed practice of participants toward using meter dose inhaler device. All
participants demonstrated correct practice regard remove the cap, hold the
inhaler device, press the dose, hold breath for 8 - 10 seconds and replace the
cap again. Also more than (80%) participants demonstrated correct during shake
the inhaler, hold it on correct position and (78%) took deep breath before
inhaled the dose. In addition to greater than (40%) of participants
demonstrated correct steps about the following items; used inhale mouthpiece
positioning, continuous breathing 3 to 5 seconds, repeating dose and rinsing
mouth with water after puff.
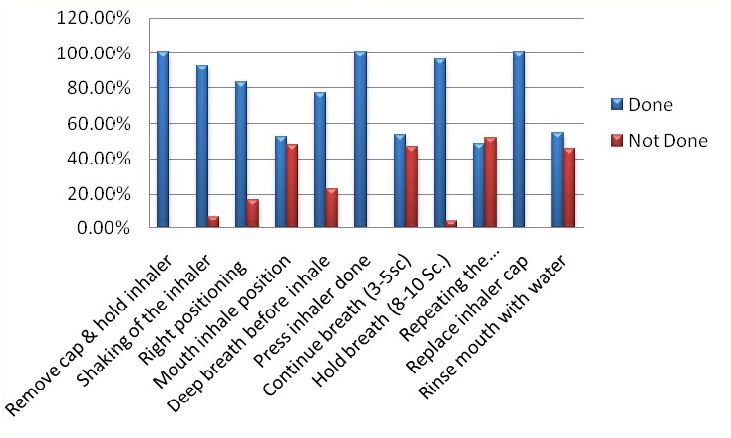
Fig.
1: Level of Participants Practice Regard Using Meter Dose Inhaler Device to
Control Bronchial Asthma (n= 105)
DISCUSSION- Asthma
is a public health problem not just for high-income countries; it occurs in all
countries regardless of the level of development. Most asthma-related deaths
occur in low- and lower-middle income countries [10,14]. The study
results reflected that more than fifty percent of the study populations were
females and above of quarter of participants their age group between 36 to 45
years. Most of them are worker and educated. In addition to 44.0 % of
participants have asthma duration for 6 to 15 years (Table 1). This study was a
similar to study conducted in 2013 at El-shaab public hospitals, to assess the
knowledge and behavior of asthmatic patients towards asthma [5].
Regard level of knowledge about meter
dose inhaler device uses the study reflected that, most of participants have a
very good knowledge about uses inhaler dose, care post inhalation, storage and
cleaning the device. While more than half of them have moderate level of
knowledge for preparing dose, replacing inhaler device and cleaning mouthpiece
and 56% of participants have very poor knowledge about mouth rinse after puff
(Table 2).
There was a highly
significance difference between the level of knowledge and education; the post
university level of education participants have highest level of knowledge
about preparation, inhalation dose, replacing and cleaning mouthpiece of meter
dose inhaler device P-values sequences are (0.000, 0.033, 0.001, 0.001), while statistically
insignificance differences about steps of inhaler dose, storage, cleaning of
meter inhaler device and rinse of mouth after puff; P values sequences are
(0.203, 0.297, 0.353, 0.242) as showed on Tables (3a & 3b). So the education has positive effect on participants knowledge this agree
with a study conducted at Bangladesh, Dhaka to assess knowledge about inhaler
use among the chronic asthma patients in selected hospitals which showed that participant’s level of
knowledge was found to be associated with their educational status.
Participants with higher education possessed more than the participants with
lower education [15]. According to Nelson Mandela “Education is most
powerful weapon which can use to change the world.” So it is very strong rational
that the higher educated persons possess more knowledge than the participants
who have lower education.
On the other hand the study reflected
that the majority off participants performed correct practice during removing
cap, inhaler device press down and replace inhaler device cap, shaking inhaler
device, right patient positioning, take deep breath before inhale and hold
breath from eight to ten seconds, while some of them had moderate practice
level for open mouth technique, continuous breathing and rinse mouth with water
after puff (Fig. 1). This
agrees with study conducted in Khartoum at El-Shaab
Teaching Hospital to assess the knowledge and behavior of asthmatic patients
towards asthma. The study showed that more than two thirds of the participants were
able to demonstrate correct use of inhaler device [5]. Also similar with study carried
in 2009 at Brazil which evaluated knowledge and techniques for using prescribed
inhalation devices among patients with asthma or COPD, which showed the 94.2%
of patients committed at least one error which showed that their technique was
inappropriate [16]
and disagree with study, which conducted in Nigeria showed that
the total percentage score of asthma knowledge significantly was satisfactory while
the demonstration of inhaler techniques was very poor [17].
CONCLUSIONS-
Most of participants had moderate knowledge about steps preparation, mouthpiece
cleaning and replacement of the inhaler device. While some of them had poor knowledge
about the benefit of oral rinsing after puff. In addition most of the
participants had very good practice about the correct use of inhaler device,
fewer of them participants had poor practicing about correct inhaler use; this
reveals the discrepancy between knowledge and practice. Proper technique is necessary in
order to achieve adequate delivery of meter dose inhaler to the lungs.
In
the future must be constructed an education programs to enhance the knowledge
for asthmatic patients regard uses of meter dose inhaler
device and encourage
care providers to use educational strategies and methods include individual
teaching, small-group sessions, large-group lectures, checklists, video and
audio tapes and booklets carried at units during patients admission
or on their clinic visit at community or make propaganda through televisions
and social media.
ACKNOWLEDGEMENTS-
Our acknowledgement for Prof. Mustafa
Numiri for advices and support, all staff at nursing college at Al- Neelain
University; Khartoum, Sudan and for the study participants and data collectors
team.
CONTRIBUTION OF AUTHORS
Research
concept- Dr.
Hassanat E. Mustafa, Mishkat S.A. Rokza
Research
design- Dr.
Hassanat E. Mustafa, Mishkat S.A. Rokza
Supervision- Dr. Hassanat E. Mustafa
Funding- Dr. Hassanat E. Mustafa, Mishkat S.A. Rokza, Badria
A. Elfaki
Materials- Dr. Hassanat E. Mustafa, Mishkat S.A. Rokza, Badria
A. Elfaki
Data
collection- Dr.
Hassanat E. Mustafa, Mishkat S.A. Rokza, Badria A. Elfaki
Data
analysis and interpretation- Dr.
Hassanat E. Mustafa, Mishkat S.A. Rokza, Badria A. Elfaki
Literature
search- Dr.
Hassanat E. Mustafa, Mishkat S.A. Rokza, Badria A. Elfaki
Writing
article- Dr.
Hassanat E. Mustafa, Mishkat S.A. Rokza, Badria A. Elfaki
Critical
review- Dr.
Hassanat E. Mustafa, Badria A. Elfaki
Article
editing- Dr.
Hassanat E. Mustafa, Badria A. Elfaki
Final approval- Dr. Hassanat E. Mustafa,
Mishkat S.A. Rokza, Badria A.
Elfaki
REFERENCES
1.
Asthm-Background.html.USA.
The New York [cited 2014 June 2]. Available from: http://health.nytimes.com/,
2013.
2.
Asthm-Background.html.USA. The New York
[cited 2014 June 2]. Available from: http://health.nytimes.com/, 2013.
3.
Asthma-Wikipedia.org.
Encyclopedia Asthma online [cited 2014 may 20]. Available from: http://en.wikipedia.org/wiki/Asthma,
2014.
4.
Asthma’s Impact.gov.
National Asthma Control Program on the Nation Data from the CDC [cited 2014
July 9]. Available from: http://www.cdc.gov/asthma/pdf, 2013
5.
South Africa world’s fourth
highest asthma death rate. GINA: health24 (Pty) Ltd; [updated 12 September
2016], 2014. 6. Ali ZT, Ahmed AH. Attitude of Patients with Bronchial Asthma
towards their Management in Alshaab Teaching Hospital Khartoum State, Sudan:
NMJ, 2013; 3(12): 13-20. 7.
Alawad AO, Khalil AH,
Merghani TH. Prevalence of Asthma among University Students and Workers.
Khartoum State, Sudan: NMJ; 2011, p. 32-38. 8.
La Sapienza University- Rome
(Italy). Metered dose inhalers and spacer devices. Department of cardiovascular
and respiratory sciences patent, 2014; 11746463. 9.
A metered-dose inhaler,
Asthma.org. The Global Conference for Wikimedia, the free encyclopedia.
Available from: http://en.wikipedia.org/wiki/ Mete
reddose_inhaler, 2014. 10. Levy ML,
Hardwell A, McKnight E, Holmes J. Asthma patients' inability to use a
pressurised metered-dose inhaler (pMDI) correctly correlates with poor asthma
control as defined by the global initiative for asthma (GINA) strategy: A
retrospective analysis. Prim Care Respir J., 2013; 22(4):
406-411. 11. Smeltzer SC, Bare BG. Brunner &Siddhartha’s Textbook of
MedicalSurgical Nursing. 10th ed., Philadelphia; Lippincott Williams
& Wilkins, 2010. 12. The University of Melbourne. Stage program designed to assist PhD,
ABN: 84 002 705 224 Graduate Centre Australia. Available from: http://gradresearch.unimelb.edu.au/,2013. 13. Mustafa HE, Elfaki BA. Determination nurses’ knowledge about
initial drugs used during emergency management of acute myocardial infarction,
JNEP, 2016; 7(5): 62-67. 14. Global Strategy for Asthma.org Management and prevention media
backgrounder. GINA. Available from: http://www.ginasthma.org/Press-Room, 2014. 15. Parvin IA, Ahmad SA, Islam MN. Knowledge about Inhaler use among
the chronic asthma patients in selected hospitals. Dhaka: Bangladesh Med Res
Counc. Bull, 2014; 3(7): 47-50. 16. Souza M L, et al. Evaluate knowledge and techniques for using
prescribed inhalation devices among patients with asthma or COPD. Bras.
Pneumol, 2009; 35(9): 824-831. 17. Desalu O, et al. Impact of Short-Term Educational Interventions on
Asthma Knowledge & metered-dose Inhaler Techniques among Post Basic Nursing
Students. Ilorin, Nigeria: Sud JMS, 2014; 8(2): 77-84.