CASE REPORT: A 40 year old lady was referred to ENT outpatient department by the physicians for hoarseness of voice. Patient had hoarseness since 10months; there was no history of smoking, alcohol abuse, voice abuse or upper respiratory tract infection. On complete ENT examination including the indirect laryngoscopy left vocal cord was found to be immobile. Other ENT examination was normal.
DISCUSSION: Hoarseness of voice due to paralysis of the left recurrent laryngeal nerve caused by a dilated left atrium in mitral stenosis was first discussed by Nobert Ortner, a Viennese physician, in1897. He explained that hoarseness was caused by compression of the left recurrent laryngeal nerve by the enlarged left atrium. Later it was described with other identifiable cardiovascular diseases associated either with left atrial enlargement including mitral regurgitation and atrial myxoma or severe pulmonary hypertension including congenital heart diseases. For this reason it is also known as cardiovocal syndrome.
CONCLUSION: For an ENT surgeon, in a case of clinical fix, when all possible causes of the vocal cord palsy are ruled out, a complete cardiovascular examination should be sought.
Key-Words- Ortners syndrome, Left recurrent laryngeal nerve palsy, Mitral stenosis, Cardiovocal syndrome
INTRODUCTION- Hoarseness of voice is a very common condition and underlying causes vary from reversible benign causes to life-threatening malignancies. Unilateral recurrent laryngeal nerve injury is most commonly caused by surgical trauma or a malignant tumor1. Cardiovocal syndrome or OrtnerÆs syndrome is hoarseness due to left recurrent laryngeal nerve palsy caused mainly by mechanical affection of the nerve from enlarged cardiovascular structures.
Cardiovocal syndrome is a rare condition and to our knowledge only 40 patients have been presented in the literature as a thorough research in Pub Med showed. It is also described to be more common in men because possibly of a higher incidence of cardiovascular conditions than in females2. Cardiovocal syndrome has a peak incidence in older age, but can occur in any age group, and it has been described even in infants3.
Hoarseness of voice is a very common symptom seen in the ENT outpatient department. While the recurrent laryngeal nerve is the most common nerve involved in the vocal cord palsy. Vocal cord palsy due to cardiac diseases and conditions are very less reported. Ortners syndrome or cardiovocal syndrome is one of it. We report a case of 40 yr female with hoarseness of voice due to severe mitral stenosis and review literature for possible cardiovascular causes of cardio vocal syndrome.
CASE REPORT- A 40 year old lady was referred to ENT outpatient department by the physicians for hoarseness of voice. Patient had hoarseness since 10months; there was no history of smoking, alcohol abuse, voice abuse or upper respiratory tract infection. On complete ENT examination including the indirect laryngoscopy left vocal cord was found to be immobile, while other ENT ex-amination was normal. To confirm this findings video laryngoscopy using a 70 degree endoscope was done and findings were confirmed (Fig 2). On retrospection patient gave history of breathlessness on exertion, occasional chest pain, and mild discomfort in swallowing solid food. On auscultation the patient had mid diastolic murmur with presystolic accentuation with opening snap in the mitral area of chest. Chest X ray PA view showed straightening of left heart border with left atrial enlargement (Fig 1). Echo cardio gram showed changes indicating left atrial enlargement with pulmonary hypertension. Cardiac echo showed stenosis of mitral valve, left atrial enlargement, pulmonary hypertension (Fig 3a & 3b). As there was no other possible explanation for the left recurrent laryngeal nerve palsy, mechanical compression of the left recurrent laryngeal nerve between the aorta and left pulmonary artery was most likely the cause. The clinical symptoms in combination with imaging findings were consistent with cardio vocal syndrome.
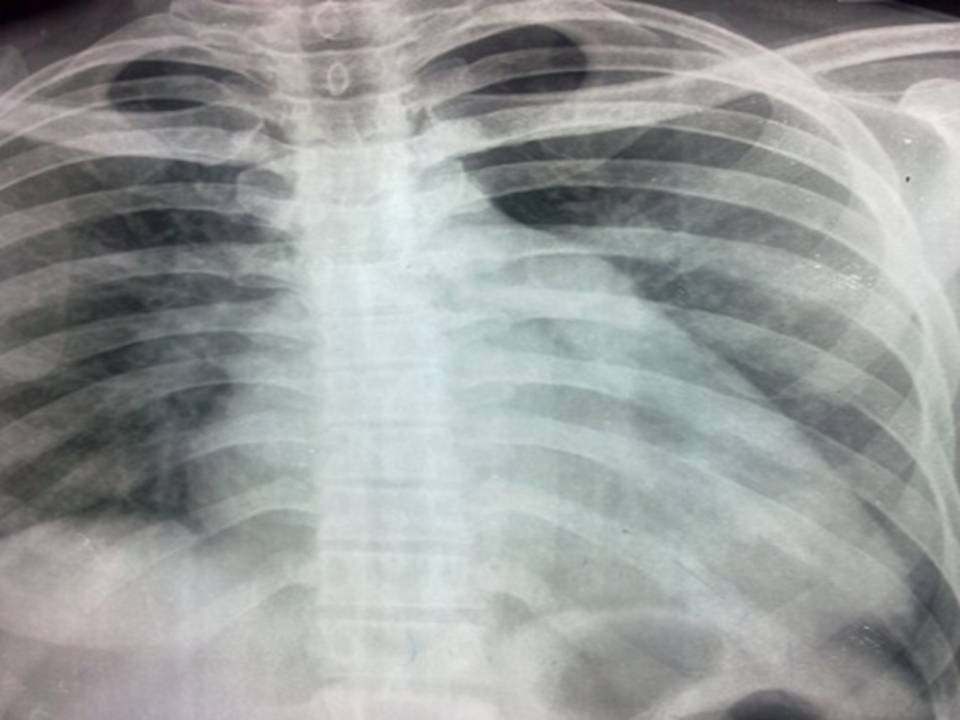
Fig 1: X-Ray Chest Pa view showing Straihtening of Left Heart Border Suggestive of Mitral stenosis
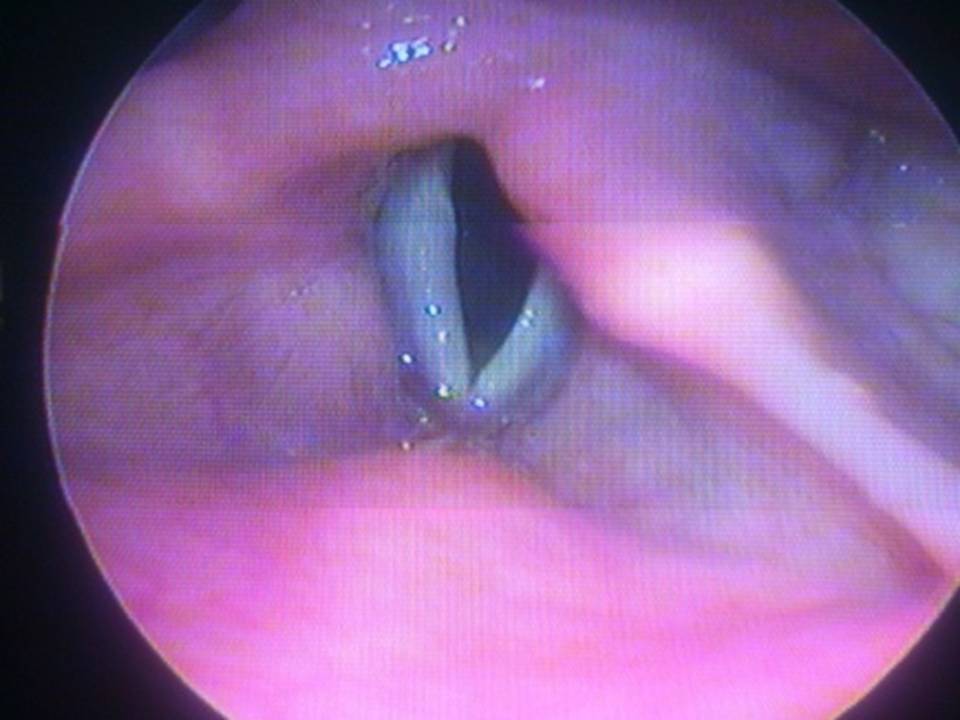
Fig 2: Videolaryngoscopy by 70o Endoscope Showing Left vocal cord palsy
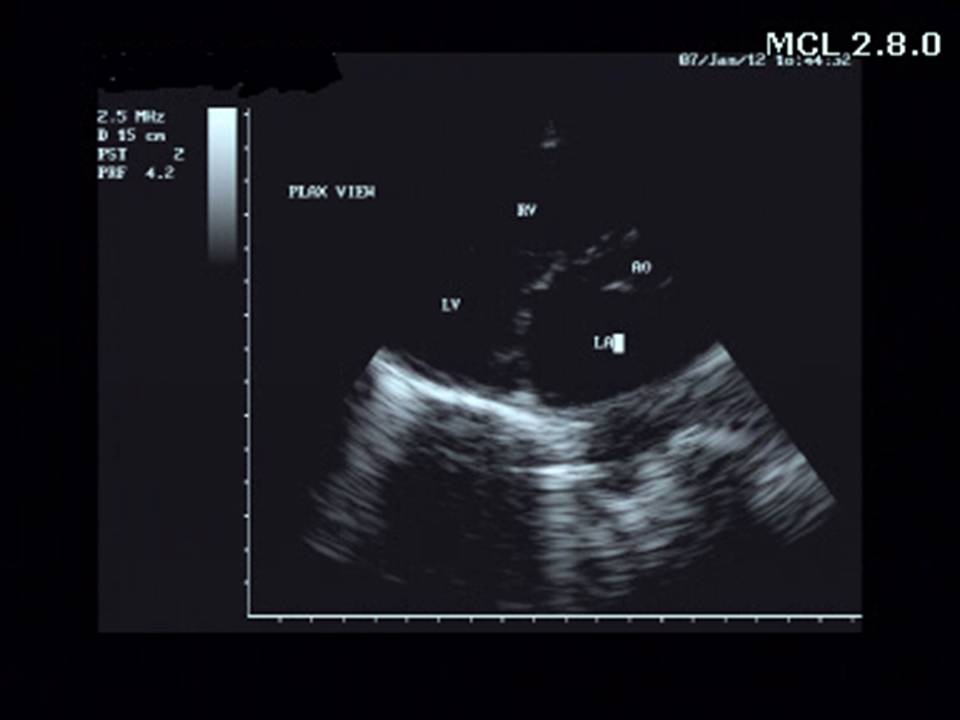
Fig 3a: 2D Echo showing left atrial enlargement with Mitral stenosis
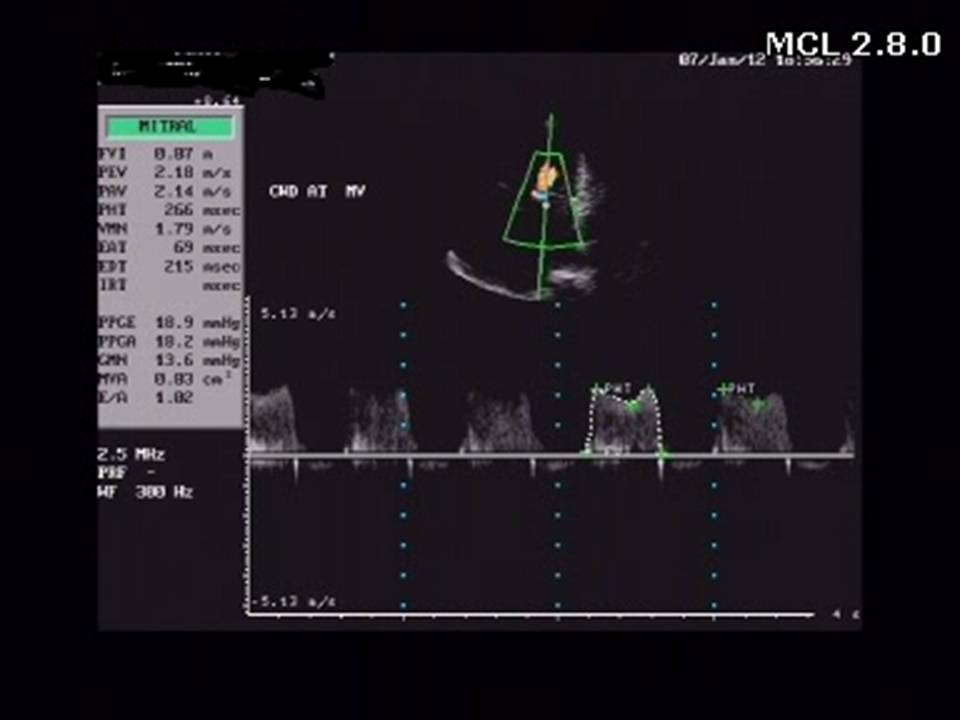
Fig 3b: 2D Echo Showing Pulmonary Hypertension
Table 1: Cardiovascular conditions associated with Ortners syndrome
| 1 | ĀĀCongenital | Atrial or Ventricular septal defect, Double outlet right ventricle, EisenmengerÆs complex, Patent ductus arteriosus, EbsteinÆs anomaly, Aortopulmonary window |
|---|---|---|
| 2 | Mitral valve disorders | Mitral stenosis, Regurgitation, Prolapsed |
| 3 | Aortic aneurysms | Saccular, Atherosclerotic, Pseudo aneurysms, Dissections, Traumatic, Mycotic |
| 4 | Adult cardiovascular disorders | Left atrial enlargement, Left ventricular aneurysm, Pulmonary hypertension, Ductus aneurysm, Pulmonary embolism, Thrombosed giant left atrium, Tortuosity of great vessels, Atrial myxoma |
| 5 | Iatrogenic | Cardiac or Thoracic surgery, Defibrillation, Atrial fibrillation Ablation procedure, Repair of Thoracic aneurysms |
| 6 | Miscellaneous | Foreign body causing oesophago-broncho-aortic fistula |
CONCLUSION- Hoarseness of voice is a very common symptom in the ENT outpatient department , caused mainly due to some ENT pathology affecting the vocal cords or the nerve directly or idiopathic causes . A complete cardiovascular examination should be sought before labeling it as idiopathic . This case is an eye opener for an ENT surgeon as such cases are rarely encountered in ENT outpatient where a cardiovascular reason leads to vocal cord palsy.
REFERENCES
- A. D. Rubin and R. T. Sataloff, ōVocal fold paresis and paralysis,ö Otolaryngologic Clinics of North America, 40:5, pp. 1109¢1131, 2007.
- S. Loughran, C. Alves, and F. B. MacGregor, ōCurrent aetiology of unilateral vocal fold paralysis in a teaching ho spital in the West of Scotland,ö Journal of Laryngology and Otology, 116:11, pp. 907¢910, 2002.
- S. A. Zaki, S. Asif, and P. Shanbag, ōOrtner syndrome in infants,ö Indian Pediatrics, vol. 47, no. 4, pp. 351¢353, 2010.
- Chan P, Lee CP, Ko JT, Hung JS. Cardiovocal (OrtnerÆs) syndrome left recurrent laryngeal nerve palsy associated with cardiovascular disease. Eur J Med 1992; 1:492-495.
- Mulpuru SK, Vasavada BC, Punukollu GK, Patel AG. Cardiovocal syndrome: a systematic review. Heart Lung Circ 2008;17:1-4.
- Ortner N. Recurrent laryngeal nerve paralysis due to mitral value stenosis, Wien Klin Wochenschr 1897;10:753¢755
- Fennessy BG, Sheahan P, McShane D. Cardiovascular hoarseness: an unusual presentation to otolaryngologists. J Laryngol Otol 2008; 122:327¢328
- Gulel O, Koprulu D, Kucuksu Z, et al. Images in car-diovascular medicine. Cardiovocal syndrome associated with huge left atrium Circulation 2007; 115:e318¢e319
- Ishimoto S, Ito K, Toyama M, et al. Vocal cord paralysis after surgery for thoracic aortic aneurysm. Chest 2002; 121:1911¢1915
- Kishan CV, Wongpraparut N, Adeleke K, et al. OrtnerÆs syndrome in association with mitral valve prolapsed, Clin Cardiol, 2000;23:295¢297.
- Nakao M, SawayamaT, SamukawaM, et al. Left recurrent laryngeal nerve palsy associated with primary pulmonary hypertension and patent ductus arteriosus,J Am Coll Cardiol 1985;5:788¢792.
- V. Subramaniam, A. Herle, N. Mohammed, and M. Thahir, ōOrtnerÆs syndrome: case series and literature review,öBrazilian Journal of Otorhinolaryngology 2011; 77:559¢562.
- M. Nakahira, H. Nakatani, and T. Takeda, ōLeft vocal cord paralysis associated with long-standing patent ductus arterio-sus,ö American Journal of Neuroradiology 2001; 22:759¢761.
| Source of Financial Support: Nil Conflict of interest: Nil |
Ā
|---|
| International Journal of Life-Sciences Scientific Research (IJLSSR) Open Access Policy Authors/Contributors are responsible for originality, contents, correct references, and ethical issues. IJLSSR publishes all articles under Creative Commons Attribution- Non-Commercial 4.0 International License (CC BY-NC). https://creativecommons.org/licenses/by-nc/4.0/ |
Ā
|---|