INTRODUCTION- Endometriosis
is a benign disease defined by the presence of endometrial glands and stroma in
anatomic locations other than the uterine lining. It is most commonly observed
in the dependent portions of the pelvis, and most frequently on the peritoneal
surfaces of the ovaries, uterosacral ligaments, and other pelvic organs.
Endometriosis can also be found anywhere in the body such as the thoracic
cavity, urinary and intestinal tracts, inguinal canal, umbilicus, surgical
scars, and the perineum. The incidence of perineal endometriosis is rare,
possibly because of underreporting. Its significance in clinical practice is
arguable. In a review of the literature, only case reports and case series have
been reported. Between 1983 and 2007, the incidence of perineal endometriosis
was 0.31% among women with endometriosis treated surgically [1]. The
rarity of cases may be because of the fact that perineal endometriosis may not
have been included in the differential diagnosis of perineal masses, which may
have led to underreporting and inadequate patient treatment.
CASE REPORT- A-25-year old woman
presented in the obstetrics and gynecology OPD at G. S. V. M. Medical College
Kanpur U.P. India with complains of perineal mass and pain for 6 months. Pain
increased during menses. She also gave a history of dyspareunia and itching
over the perineal region. There was a history of vaginal delivery with
episiotomy 1 year back. On local, examination a mass was present at perineum
near the episiotomy site. On the basis of history and examination scar
endometriosis mass suspected. After routine laboratory investigation, surgical
excision of the mass was done under spinal anesthesia and the specimen was sent
to the pathology department for histopathological examination.
Gross
findings- Specimen consists of multiple greyish white to
greyish brown soft to firm tissue pieces altogether measuring 2x1.5 cm. Whole
tissue was processed. Paraffin blocks made and tissue sections
were stained with hematoxylin and eosin for microscopic examination.
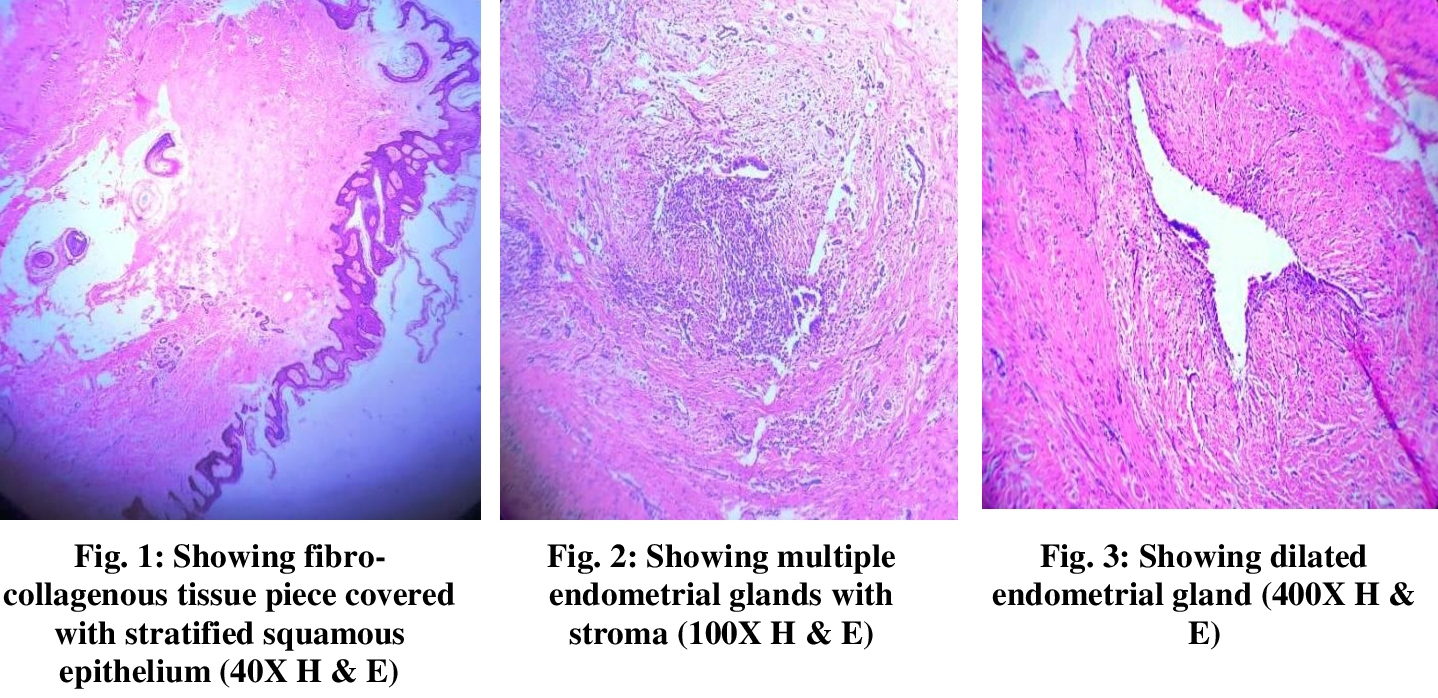
Microscopic
findings- Section shows fragmented tissue piece lined by
keratinized, hyperplastic stratified squamous epithelium. Underlying
fibro-collagenous stroma shows few endometrial glands with scanty stroma.
Glands are lined with low columnar epithelial cells. A Section also shows
multiple hair follicles, pilosebaceous units, multiple small proliferating
thin-walled blood vessels, subcutaneous fatty tissue and dense inflammatory
cell infiltrate comprising of lymphocytes, macrophages, and neutrophlis. One
cystic space seen lined by low cuboidal to flattened epithelium filled with
hemorrhage and inflammatory cell infiltrate comprising of lymphocytes,
macrophages, and neutrophlis. Few smooth muscle bundles are also seen.
DISCUSSION- Scar endometriosis is a
rare entity. The incidence has been estimated to be only 0.03–0.15 % of
all cases of endometriosis [1]. The incidence of episiotomy scar
endometriosis was estimated to be 15 of 2028 consecutive deliveries [2].
Patil et al. [3] studied
17 cases of extrapelvic endometriosis in a time span of 15 years and found
a total of three cases of episiotomy scar endometriosis. Luterek et al. [4] reported a case of
a 33-year-old woman with a medical history of recurrent perianal endometriosis.
An endometriotic giant mass (8 cm in diameter) was widely excised together
with the episiotomy scar. They concluded that a wide excision is mandatory as
it is the only way to prevent tumor recurrence.
Treatment of choice is wide excision of the lesion and medical management if required. Only medical treatment with the use of progestogen, oral contraceptive pills, and danazol is not effective and gives only partial relief in symptoms. Recently, there has been a report of use of gonadotropins agonist but only with prompt improvement in symptoms with no change in the lesion size. These patients need to be followed up because of the chances of recurrence, which require re-excision. In the case of continual recurrence, the possibility of malignancy should be kept in mind [5].
A
tender nodule or perineal mass, accompanied by progressive and cyclic perineal
pain in a patient with a history of an episiotomy, is highly diagnostic [6].
Physical examination usually reveals a tender bluish perineal mass. Previously
reported cases consistently describe these physical exam\ findings. Symptoms
usually appear shortly after ectopic endometrial cell implantation, with some
cases having a prolonged latent period of up to 14 years after implantation [7].
CONCLUSIONS-
The perineal scar endometriosis was confirmed by histopathological examination.
Patient was asymptomatic since surgical management. We had reported this case
because of rare incidence and perineal scar endometriosis should be included in
the differential diagnosis of perineal masses if associated with cyclical pain
and a history of childbirth so that adequate treatment and follow-up can be
done.
ACKNOWLEDGEMENTS-
All authors very thankful to the Department of
Pathology, G.S.V.M. Medical College Kanpur, India for help in writing the
paper.
CONTRIBUTION OF AUTHORS
Research concept- Dr. Mahendra Singh, Dr. Jagdish kumar
Research design- Dr. Jagdish kumar
Supervision- Dr. Mahendra Singh
Materials- Dr. Anita Omhare, Dr. Neelima Verma
Data collection- Dr. Jagdish kumar
Data analysis- Dr. Jagdish kumar
Literature search- Dr. Jagdish kumar
Writing article- Dr. Jagdish kumar
Critical review- Dr. Mahendra Singh
Article editing- Dr. Anita Omhare, Dr. Neelima Verma
Final approval- Dr. Mahendra Singh, Dr. Jagdish kumar
REFERENCES
1.
Francica G, Giardiello C, Angelone G, et
al. Abdominal wall endometriosis near cesarean delivery scars. J.
Ultrasound Med., 2003; 22: 1041–47.
2.
Paul T, Tedeschi LG. Perineal
endometriosisat the site of episiotomy scar. Obstet. Gynecol., 1972;
40: 28–34.
3.
Patil BS, Tripathi JB, Patil FB, et al.
Extrapelvic endometriosis: A study of 17 cases. J. South Asian Fed.
Obster. Gynecol., 2012; 4(1): 32–34.
4.
Luterek K, Barcz E, Bablok L, et al.
Giant recurrent perineal endometriosis in an episiotomy scar- A case
report. Ginekol. Pol., 2013; 84(8): 726–29.
5.
Park SW, Hong SM, Wu HG, et al. Clear
cell carcinoma arising in a cesarean section scar endometriosis. J. Korean
Med. Sci., 1999; 14: 217–19.
6.
Zhu L, Lang JH, Xin F, et al. The diagnosis
and treatment of perineal endometriosis. Chin. J. Obstet. Gynecol., 2002; 37:
53-64.
7.
Kinkel K, Frei KA, Balleyguier C, Chapron C.
Diagnosis of endometriosis with imaging: A review. Eur. Radiol. 2006; 16: 285-98.