ABSTRACT- Introduction: Low back pain (LBP) is an important clinical, social, economic, and public health problem
affecting the population indiscriminately. It is a disorder with many possible etiologies, occurring in many groups of the
population, and with many definitions. Nearly everyone will experience some form of back pain in his or her lifetime.
Materials ans& Methods: The current study is a cross sectional study undertaken at Lord Buddha Koshi Medical
College, Saharsa, Bihar, India from Aug 2015 to Dec 2015. The objective of this study was to see the age specific
prevalence of low back pain among 400 subjects visiting the Orthopedics OPD of the hospital. The age range of the study
participants were 25 years to 65 years. The national guidelines of LBP diagnosis is used as diagnostic criteria.
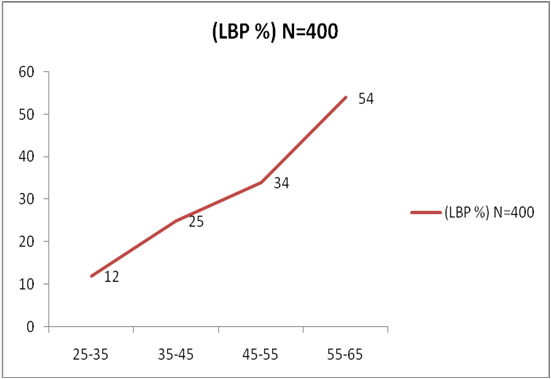
Results: Overall prevalence of LBP was found as 31.25%. The highest prevalence was seen in 55-65 years age group.
Age had positive association & important risk factors of increasing burden of LBP.
Conclusion: LBP is an important health problem & affecting all age groups and it is responsible for a great economic loss
of any country.
Key-words- Low Back Pain, Prevalence, Public Health
INTRODUCTION-
Low back pain (LBP) is an important clinical, social,
economic, and public health problem affecting the
population indiscriminately. It is a disorder with many
possible etiologies, occurring in many groups of the
population, and with many definitions [1]. Nearly everyone
will experience some form of back pain in his or her
lifetime. The low back is the area behind the belly from the
rib cage to the pelvis and is also called the lumbar region.
Back pain is a major cause of missed work. Low back pain
usually resolves on its own and is commonly the result of a
strain injury. There are many treatments for low back pain
[2]. Men and women are equally affected by low back pain,
which can range in intensity from a dull, constant ache to a
sudden, sharp sensation that leaves the person
incapacitated. Pain can begin abruptly as a result of an
accident or by lifting something heavy, or it can develop
over time due to age-related changes of the spine [3].
Consequently, the vast literature available on LBP is not
only heterogeneous but also contradictory [1]. In accordance
with the report of World Health Organization in 2002, LBP
constituted 37% of all occupational risk factors which
occupies first rank among the disease complications caused
by work. Such high prevalence of complications at
international levels has made the World Health
Organization to name the first decade of the third
millennium as the “decade of campaign against
musculoskeletal disorders (as the silent epidemic)” (WHO,
2005). Sedentary lifestyles also can set the stage for low
back pain, especially when a weekday routine of getting too
little exercise is punctuated by strenuous weekend workout
[3]. Most low back pain is acute or short term, and lasts a
few days to a few weeks [4]. Low back pain is a leading
cause of disability [5]. It occurs in similar proportions in all
cultures, interferes with quality of life and work
performance, and is the most common reason for medical
consultations. Few cases of back pain are due to specific
causes; most cases are non-specific. Acute back pain is the
most common presentation and is usually self-limiting,
lasting less than three months regardless of treatment.
Chronic back pain is a more difficult problem, which often
has strong psychological overlay: work dissatisfaction,
boredom, and a generous compensation system contribute
to it. It tends to resolve on it’s own with self-care and there
is no residual loss of function [6]. The majority of acute low
back pain is mechanical in nature, meaning that there is a
disruption in the way the components of the back (spine,
muscle, inter-vertebral discs, and nerves) fit together and
move [3]. For arbitrary classification purposes, chronic pain
generally is defined as pain that has persisted beyond
normal tissue healing time (or about three months) [7].
Chronic back pain is also defined as pain that persists for
12 weeks or longer, even after an initial injury or
underlying cause of acute low back pain has been treated [3].
However, more recent reports from [8-12] suggest that
prevalence rates are not that dissimilar from Western
countries with one year prevalence in adults in these studies
between 36% and 64%. A study done on truck drivers by
[13] the prevalence was 62%. Another study of [14] for
general population shows 34.21%.
In the present papers an attempt was made to see the
prevalence/Incidence of Low back patients in a tertiary care
hospital and the spectrum of age groups of those patients.
MATERIALS AND METHODS-
The current study is a cross sectional study undertaken at
Lord Buddha Koshi Medical College, Saharsa, Bihar, India
from Aug 2015 to Dec 2015. The objective of the study
was to see the age specific prevalence of low back pain.
The age range of the study participants is 25 years to 65.
All the patients visiting Orthopedic OPD of the hospital &
want to participate in the study was taken. Those patients
who shown some other kinds of morbidity with chronic
disease were excluded from the study. The hypothesis of
the study was the prevalence of the LBP is very alarming
and is most common in a particular age group. The sample
size was calculated by the help of Statistician by using:
N = total sample size (number of experimental units)
P = Prevalence of metabolic disorder (50 % Taken because exactly not known in the current time and study region)
Q=1-P (50%)
Z(1-(a/2)= related to the chosen significance criterion a; can be found in normal distribution tables, (1.96)
?: relative precision (10% is taken in the present study)
Above formula gives, N=384 which is the minimum sample size required for the current study
A random sampling technique is used to collect the sample. The data was analyzed by using SPSS 20.0 (IBM Chicago). The frequency & percentage was calculated for categorical data whereas the mean & standard deviation was calculated for continuous data.
RESULTS- The frequency of study variables of the study subjects is represented in Table 1. Among 400 study subjects, mean age of study subjects were 40 (±11.19) years. The total numbers of male subjects were 210 (52%) & females were 190 (48%). The 52% subjects were from urban area while 48% were living in rural area. The 73% study subjects were literate. Almost half proportion was found from high economic class family. Almost 48% people reported that they are smokers.
Table 1: Study variables of the study subject
| S. No. | Variable | N | % |
|---|---|---|---|
The age specific prevalence of Low Back Pain (LBP) is shown by table 2. All the study subjects were divided in four study groups (represented in Table 2) of equal frequencies of 100 i.e. age matched criterion then on the basis of diagnostic criterion of low back pain (LBP) national clinical guidelines.
Table 2: Age specific prevalence of Low Back Pain (LBP)
| S. No. | Age Specific Prevalence | (LBP %) N=400 |
|---|---|---|
Summary of recommendations of 11 national clinical guidelines for acute low back pain [15]
Diagnosis-
- Diagnostic triage (non-specific low back pain, radicular syndrome, specific pathology)
- History taking and physical examination to exclude red flags
- Physical examination for neurological screening (including straight leg raising test)
- Consider psychosocial factors if there is no improvement
- X- Rays not useful for non-specific low back pain
DISCUSSION- Previous study was also found better results of matched treatments in sub-groups of patients with non-specific low back pain. The high prevalence of LBP among farmers is most likely the result of injury to the spinal structures, which may arise from working postures and movements of the lower back during the work process. This study demonstrated the point prevalence of LBP and associated factors among Thai farmers during the rice transplanting process. Regarding the aspects of prevalence stratified by personal characteristics, farming characteristics, and stress levels, the results of the current study showed that the prevalence of LBP was significantly higher in the farmers with high or severe stress levels. This result confirms that farmers with high stress were more likely to have LBP. In the current study, the prevalence of stress among females was slightly higher than in males, but this was not significant. This result is consistent with a previous study that reported that the prevalence of LBP was not differentiated by gender. LBP disorders may occur due to many factors. Previous studies have reported that the personal characteristics associated with LBP were age, BMI, exercise, alcohol consumption, and smoking. In the present study, only age was related to LBP, which confirms results from some previous studies.
CONCLUSION- In the present study LBP prevalence was found in different age groups and its significance is also mentioned. LBP is an important health problem & affecting all age groups and responsible for a great economic loss of any country.
- REFERENCES-
| International Journal of Life-Sciences Scientific Research (IJLSSR)
Open Access Policy Authors/Contributors are responsible for originality, contents, correct references, and ethical issues. IJLSSR publishes all articles under Creative Commons Attribution- Non-Commercial 4.0 International License (CC BY-NC). https://creativecommons.org/licenses/by-nc/4.0/legalcode |
| How to cite this article: Sinha AP: Age Specific Prevalence of Low Back Pain: A Hospital Based Cross-sectional Study. Int. J. Life. Sci. Scienti. Res., 2017; 3(2): 932-935. DOI:10.21276/ijlssr.2017.3.2.10 Source of Financial Support: Nil, Conflict of interest: Nil |